Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124
Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

BBC Africa Health Correspondent, Lagos
 Ghetto images
Ghetto imagesAt the age of 24, Nafis Salahu was in danger of becoming just another statistics in Nigeria, where a woman died, giving birth every seven minutes.
Entering birth during the strike of doctors meant that although he was in hospital, there was no expert assistance after a complication arose.
Her baby’s head was stuck and it was just said to lie still during birth, which lasted three days.
In the end, a caesarean section was recommended and there was a doctor who was ready to perform it.
“I thanked God because I was almost dying. I was left with no strength, there was nothing left,” G -ja Salahu tells the BBC from Kano in the northern part of the country.
She survived, but tragically her baby died.
Eleven years onwards, she has returned to the hospital to give birth several times and occupy a fatalistic attitude. “I knew (every time) that I was between life and death, but I was no longer afraid,” she says.
The experience of d -jj Salahu is not uncommon.
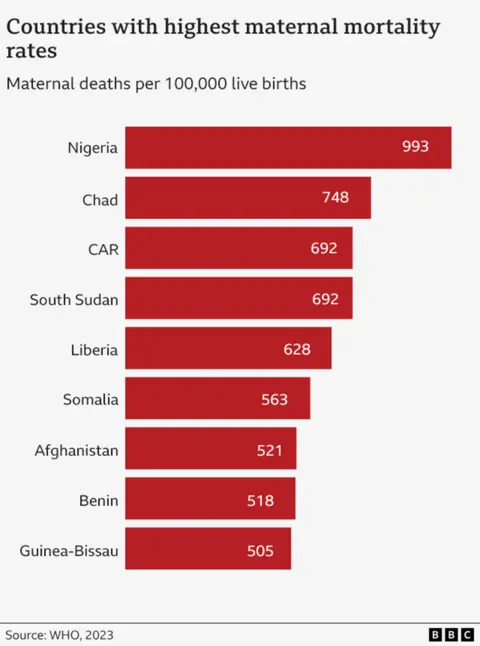
Nigeria is the most dangerous nation in the world to be born.
According to UN most estimates for the countryComposed of numbers 2023, one in 100 women died at work or in the coming days.
This puts it on top of the league table that no country wants to target.
In 2023, Nigeria represented well over a quarter – 29% – of all mother’s deaths around the world.
This is approximately a total of 75,000 women who die at birth for one year, which works at one death every seven minutes.
Warning: This article contains an image depicting a newborn baby.
 Henry Edeh
Henry EdehThe powerlessness for many is that a large number of deaths – from things like bleeding after birth (known as birth after birth) – are preventable.
Chinenye Nweze was 36 years old when she swayed at a hospital in the southeastern city of Onisha five years ago.
“Doctors needed blood,” Brother Henry Edeh recalls. “The blood they had was not enough, and they were running around. The loss of my sister and my friend is nothing I would wish for an enemy. The pain is unbearable.”
Other common causes of the mother’s death are prevented labor, high blood pressure and dangerous abortions.
“The very high” percentage of Nigeria’s maternal mortality rate is the result of a combination of a number of factors, according to Martin Dolten of the Nigeria office of the UN Child Organization, UNICEF.
These, in their view, are poor health infrastructure, a shortage of medics, expensive treatments that many cannot afford, cultural practices that can lead to some distrustful medical professionals and uncertainty.
“No woman deserves to die while giving birth to a child,” says Mabel Onwema, a national coordinator of the Women’s Development Foundation at the goal.
She explains that some women, especially in rural areas, believe that “the visit to hospitals is a complete waste of time” and choose “traditional medicines instead of seeking medical help, which can delay life -saving care.”
For some, reaching a hospital or clinic is almost impossible due to lack of transport, but Mrs. Onwuemena believes that even if they have succeeded, their problems will not be over.
“Many healthcare facilities lack the basic equipment, consumables and trained staff, which makes it difficult to provide quality service.”
Currently, the Federal Government of Nigeria spends only 5% of its health budget – far from 15% the goal with which the country is committed to a 2001 African Union treaty.
In 2021, there were 121,000 midwives for a population of 218 million and less than half of all births were observed by a qualified health worker. It is estimated that the country needs 700,000 more nurses and midwives to meet the recommended ratio of the World Health Organization.
There is also a severe lack of doctors.
The shortage of staff and facilities delays some of the search for professional assistance.
“To be honest, I don’t believe much in hospitals. There are too many stories of negligence, especially in public hospitals,” says Jamila Ishak.
“For example, when I had my fourth child, there were complications at birth. The local fertility employee advised us to go to the hospital, but when we got there, there was no health worker to help me. I had to go back home and eventually gave birth there,” she explains.
The 28-year-old from Kano is now expecting her fifth baby.
She added that she would think to go to a private clinic, but the price is excessive.
Chinwendu Obiejesi, who is expecting her third child, is able to pay for private health care at a hospital and “would not think of giving birth anywhere else.”
She says that among her friends and family, the death of her mother is already rare as she has heard about them quite often.
She lives in the rich suburb of Abuzha, where hospitals are easier to reach, the roads are better and the emergency services work. More women in the city are also educated and know the importance of going to the hospital.
“I always visit antenatal care … This allows me to talk regularly with doctors, do important tests and scans and follow both my health and the baby,” G -Ja Obiejesi told the BBC.
“For example, during my second pregnancy, they expected that I could bleed hard, so they prepared extra blood in the event that a transfusion was needed. Fortunately, I didn’t need it and everything went well.”
However, her family friend was not so lucky.
During her second work, “The birthmother could not deliver the baby and tried to expel him. The baby died. By the time she was taken to the hospital, it was too late. She still had to undergo surgery to deliver the baby’s body. She was a broken heart.”
 Ghetto images
Ghetto imagesDr. Nana Sandah-Abubar, Director of Community Health Services at the National Primary Health Development Agency (NPHCDA), admits that the situation is terrible, but says a new plan is being created to deal with some of the problems.
Last November, the Nigerian Government launched the pilot phase of the Innovation Initiative to reduce the mortality rate of the mother (MAMII). In the end, this will be directed to 172 areas of local self -government in 33 states, representing more than half of all birth -related deaths in the country.
“We identify every pregnant woman, know where she lives and support her through pregnancy, birth and beyond,” says Dr. Sanda-Abubar.
So far, in 400,000 pregnant women in six states have been found in a house in house in house, “with details whether they visit Ante-Ravni (classes).”
“The plan is to start connecting them to services to ensure that they get care (need) and that they deliver safely.”
Mamii will strive to work with local transport networks to try to make more women in clinics, and will also encourage people to register with low -cost public health insurance.
It is too early to say if this has had any impact, but the authorities hope that the country can ultimately follow the trend of the rest of the world.
Globally, the mother’s death has dropped by 40% since 2000, thanks to extension of health care. The numbers also improved in Nigeria over the same period – but only by 13%.
Despite MAMII and other programs, such as welcome initiatives, some experts believe that more need to be made – including more bigger investment.
“Their success depends on prolonged funding, effective implementation and continuous monitoring to ensure that the envisaged results have been achieved,” says Unicef Dohlsten.
Meanwhile, the loss of every mother in Nigeria – 200 every day – will continue to be a tragedy for the participating families.
For d -Edeh, the grief is still harsh because of the loss of his sister.
“It is activated to become our anchor and spine because we lost our parents when we grew up,” he says.
“In my lonely time when it crosses my mind. I cry bitterly.”
 Getty Images/BBC
Getty Images/BBC